The term amniotic band syndrome is applied to a broad spectrum of sporadic congenital anomalies that involve the limbs, craniofacial regions, and trunk, ranging from constrictive bands, pseudosyndactyly to amputation, as well as multiple craniofacial, visceral, and body wall defects (1-8). The term amniotic band syndrome also encompasses amniotic band disruption complex (3), amniochorionic mesoblastic fibrous strings (1), aberrant tissue bands (2), amniotic deformity, adhesion and mutilation (ADAM) complex (9,10), amniotic adhesion malformation syndrome (11), and the limb body wall complex (12). It has been suggested that the term syndrome is inappropriate and a more correct term for amniotic band-associated anomalies is amniotic band sequence (ABS) as they are thought to occur as a consequence of amniotic bands.
ABS is associated with numerous antenatal sonographic features, as there are numerous forms of the syndrome and these features may occur as isolated problems or in combination. The earliest that amniotic bands have been seen is at 12 weeks of gestation, by endovaginal probe. The bands can be extremely difficult to detect sonographically and ABS is more often diagnosed by the effect that they have on fetal anatomy.
The effect of amniotic bands on the extremities may be manifested by absent digits or portions of limbs, or a swollen distal arm or leg resulting from constrictive amniotic bands (42).
ABS may affect the face with cleft lip or palate, asymmetric microphthalmia, or severe nasal deformity. Encephalocele may be a manifestation of ABS, especially when off-midline eccentrically placed.
Abdominal wall defects can be the result of ABS, typically with large defects with free-floating intestine herniated outside the abdomen. The characteristic appearance of an aberrant sheet or band of amnion attached to the fetus with resultant deformity and restriction of motion allows a diagnosis of ABS to be made (Figure 3). However, prenatal diagnosis is the exception rather than the rule.
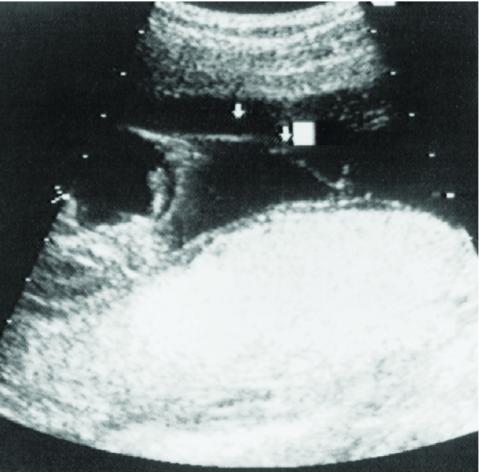
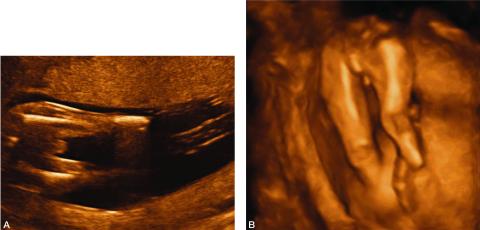
Figure 1: Sonographic image demonstrating an amniotic band attached to the fetus and floating in the amniotic fluid.
Figure 2. A. 2-D image depicting amputation of the distal portion of both lower extremities as a result of amniotic bands.
B. 3-D image of the same fetus showing bilateral limb reduction defects.
The findings in ABS may be limited to isolated defects, including isolated facial cleft, digital amputation, or mild elephantiasis of an extremity beyond a constrictive band (43,44). These isolated features may be difficult to diagnose sonographically because the detailed fetal visualization required is beyond the scope of routine obstetrical ultrasound examinations. At the worst end of the spectrum, the fetus may be so severely deformed by the amniotic bands that the spine is contracted and organs are formed in perplexing and bizarre proportions. The head may be completely misshapen or absent. The bands responsible for these deformities are rarely seen and a presumptive diagnosis of ABS is made based on the commonly associated deformities.
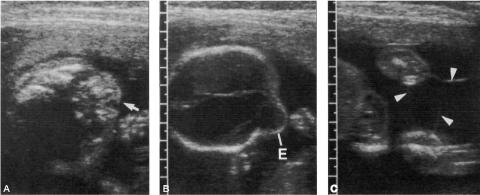
Figure 3: Sonographic image of a fetus with amniotic band syndrome manifesting as:
A. a ‘‘slash” defect in the maxillary region, and
B. an eccentric encephalocele.
C. Amniotic bands were also noted to be attached to the extremities (arrowheads).
The spinal deformities in ABS can be severe, manifesting as kyphotic lordosis or scoliosis as well as severe rotational abnormalities and even spinal amputation (45). While spinal deformity can be seen in other syndromes, severe spinal deformity should suggest ABS.
Spinal deformity associated with an abdominal wall defect is particularly suggestive of ABS. While the typical appearance of an omphalocele is possible, the more common defect is a large slashlike defect of both the thoracic and abdominal cavities with evisceration. These defects are associated with exteriorized bowel, liver, and sometimes heart without an enveloping membrane. When associated with limb abnormalities, this is characteristic of the LBWC form of ABS.
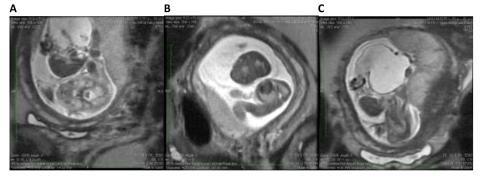
Figure 4. Fetal MRI of a fetus with limb–body wall complex showing severe twisting deformity of the spine associated with abdominoschisis and amniotic bands attached to the extremities.
A. The fetal MRI image demonstrates the contorted position of the fetus which in the same plane shows the axial view of the head and the adjacent completely extracorporeal liver and small bowel.
B. The fetal MRI image shows the fetal chest in axial plane demonstrating the very tiny chest and hypoplastic lungs.
C. The image shows the very short two vessel cord going from the large cystic structure which replaced the abdominal cavity directly into the placenta. These findings are most consistent with limb body wall complex.
Deformation of the calvarium is another group of anomalies characteristic of ABS. If complete, the fetus may appear anencephalic or to have acrania (46). If partial, the fetus may appear to have an encephalocele. The distinguishing features that characterize these defects as ABS are their asymmetric nature and associated spinal deformity or abdominal wall defects. In classic anencephaly, the calvarial bones are symmetrically absent. In anencephaly caused by ABS, there is some portion of calvarium present, usually near the base of the skull or near one or the other orbit. Similarly, classic encephaloceles occur near the midline, while ABS causes encephaloceles off the midline.
The presence of bands is unnecessary for the diagnosis of ABS in the presence of characteristic fetal anomalies. The sonographic detection of bands is helpful in confirming the diagnosis of ABS as the cause of fetal deformity. However, observation of these bands without fetal abnormality is not ABS. It is important for the sonographer to distinguish amniotic bands from other membranes and separations within the amnion. Separation of amnion and chorion is normal in early pregnancy until fusion occurs at approximately 16 weeks of gestation (47-49).
Chorioamniotic separation may occur as a result of amniocentesis or fetal surgery, and extrachorionic hemorrhage may separate the chorioamniotic membrane from the uterine wall (39,48,50). In both of these instances, a membrane may be observed sonographically. Other causes of membranes in the developing fetus include septate uterus, blighted twin, and circumvallate placenta (51).
Adhesions that form in the uterus as a result of curettage, cesarean section, or myomectomy may cause sheets of amnion that protrude into the lumen of the amniotic cavity (51-55). Randal et al., found that 76% of patients with amniotic sheets had undergone prior instrumentation (55). This results in an adhesion that becomes covered by chorion and amnion and has a thickness similar to the intertwin membrane of dichorionic diamniotic twins. These amniotic sheets do not adhere to the fetus because the amnion is intact (56). The uterine adhesion may rupture with growth of the fetus. Filly and Golbus have described the sonographic appearance of these synechiae as having a thickened base and a fine edge that undulates (51). There may be a bulbous edge, presumably due to the synechiae. There are no associated fetal abnormalities, and there is free fetal movement around the sheet. The synechiae may not be seen in the third trimester, because of rupture or compression by the growing fetus.
In the LBWC, there is a constellation of abnormalities, including myelomeningocele or caudal regression, thoracoabdominoschisis, or abdominoschisis and limb defects.
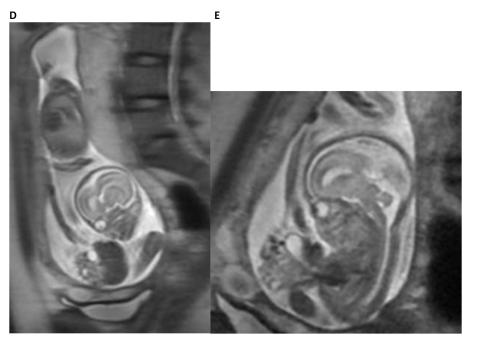
Figure 4. Fetal MRI of a fetus with limb–body wall complex showing severe twisting deformity of the spine associated with abdominoschisis and amniotic bands attached to the extremities.
D. The fetal MRI image demonstrates the contorted position of the fetus with the sagittal view of the head and the immediately adjacent completely extracorporeal liver, stomach and small bowel. In addition, the foreshortened two vessel umbilical cord is also seen in its entirety.
E. The fetal MRI image shows the fetal abdomen and chest in axial plane demonstrating the very tiny chest and herniated liver, stomach, small and large bowel with foreshortened umbilical cord. These findings are most consistent with limb body wall complex.
At least two of the three abnormalities listed above are necessary to make a diagnosis of LBWC. In LBWC, the umbilical cord is usually short but present. In body stalk anomaly, a similar constellation of findings may be seen but the umbilical cord is absent with the placenta attached directly to the fetus. If present in LBWC, there may be only a two-vessel cord. The limbs may be missing or the feet clubbed. The spine is often short and curved and sacral regression is common. There may be Arnold–Chiari malformation and hydrocephalus associated with the meningomyelocele. There may be ectopia cordis as part of the thoracoabdominoschisis. Facial clefts may also be seen in LBWC.
ABS involving the umbilical cord can be recognized by abnormal clustering of loops of umbilical cord entangled by a band, which may also be adherent to a limb. The cluster of umbilical cord loops will move together with movement of the involved limb. These findings may be subtle and should be sought in any case of ABS as umbilical cord involvement may result in fetal demise.
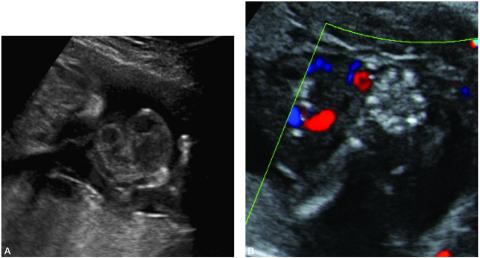
Figure 5. A. Sonographic image of amniotic bands involving the umbilical cord and the right hand and upper extremity. Movement of the hand would cause a cluster of umbilical cord loops to move together indicating amniotic band involvement of the umbilical cord.
B. Color Doppler of the same patient.
Extremity ABS should be assessed by pulse-wave and color Doppler to determine the severity of vascular compromise. Some constrictive bands may reduce the pulsatile blood flow distal to the band suggesting threatened limb loss.
Magnetic resonance imaging is an important adjunctive imaging technique which may provide more detailed information about the abnormalities which may help confirm the diagnosis or suggest alternative diagnoses (57,58). The wide field of view provided by MRI also provides assistance in planning the operative approach to fetoscopic lysis of amniotic bands.
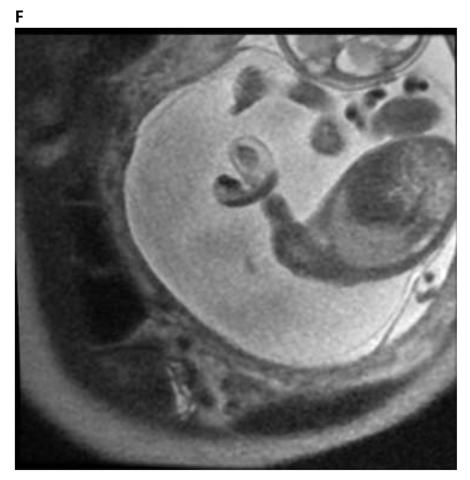
Figure 4. F. The fetal MRI image shows the effects of a constrictive amniotic band on the left upper extremities at the distal upper arm with distal edema. The Image also shows the umbilical cord in close proximity to the area of constriction suggesting umbilical cord involvement in amniotic band syndrome.
In cases of ABS involving encephalocele, fetal MRI plays an important role in evaluating the involvement of brain tissue, structural abnormalities and herniation in the encephalocele (58). Fetal MRI may also be helpful in assessing facial clefts in which may be difficult to determine the full extent of the clefting on ultrasound alone. Fetal MRI can also be used to measure fetal lung volumes in cases of abdominoschisis or thoracoshisis in which the lung development may be compromised causing severe pulmonary hypoplasia (60,61). This information may aid counseling of parents regarding prognosis and decisions around newborn resuscitation.
There is great controversy about the pathogenesis of the various forms of ABS. Part of this controversy involves the timing in gestation of the development of amniotic bands. However, in constrictive amniotic bands of the extremities, the progression of constriction combined with fetal growth has resulted in extremity amputation (65-68).
Figure 2. A. 2-D image depicting amputation of the distal portion of both lower extremities as a result of amniotic bands.
B. 3-D image of the same fetus showing bilateral limb reduction defects.
ABS can be associated with either polyhydramnios or oligohydramnios. Despite the severity of some forms of ABS, there are no adverse maternal consequences for this diagnosis. The incidence of intrauterine fetal death from ABS involving the umbilical cord is not known but numerous cases have been reported (1,39,69). However, the poorly characterized pathogenesis of this syndrome and limited sonographic surveillance, limit our understanding of its prenatal natural history.
ABS is a relatively common, if underappreciated, cause of fetal and neonatal morbidity and mortality. The fetal lamb model of ABS has been useful to define the pathophysiology of ABS and to provide a tool to understand the unique fetal response to tissue injury, repair, and regeneration. Sonographic identification of ABS affecting the umbilical cord may be an indication for fetoscopic surgical intervention. Intervention for nonlethal limb deformation may also be considered if maternal risk is sufficiently low. ABS is another in a growing list of conditions for which fetal surgery may be considered.
Constrictive bands most commonly affect the extremities, but can also involve the umbilical cord, with resulting fetal death. Kanayama et al., described the reversal of diastolic flow observed in a fetus with umbilical cord constriction due to amniotic bands (69). Graf et al. (1997) similarly reported a case of amniotic bands involving the umbilical cord following the development of chorioamniotic separation (39). Despite initially normal umbilical artery Doppler waveforms, this fetus died within 2 weeks from a constrictive amniotic band of the umbilical cord. Reports have described constrictive amniotic bands as a cause of fetal death (1,14). However, until the reports by Kanayama and Graf and their colleagues, this was a diagnosis made pathologically after the fact. It is in cases like these, fetoscopic lysis of amniotic bands can be lifesaving (see Fetal Intervention below) (39,69). Cases of ABS, by definition, have disrupted membranes and typically deliver prematurely at 32-36 weeks.
The indications for fetal surgery are, with few exceptions, only for life-threatening conditions such as congenital pulmonary airway malformation (CPAM) with hydrops, diaphragmatic hernia with a low lung-to-heart ratio, bladder outlet obstruction with oligohydramnios, or sacrococcygeal teratoma with hydrops.
However, as experience with the techniques of fetal surgery has grown and the natural histories of certain non-life-threatening conditions have been better defined, the indications for fetal surgery have been extended. Two examples of this are in utero repair of meningomyelocele to prevent the devastating neurologic injury to the spinal cord (70) and fetoscopic cord ligation in monochorionic twins with imminent death of one twin to preserve the life and neurologic integrity of the surviving twin (71). The indications for fetal surgery in the ABS may be either for a life-threatening condition if it involves constriction of the umbilical cord or, more commonly, threatened limb amputation due to amniotic band constriction of the extremity (1,72-86).
Torpin reported 36 cases of fetal death due to cord constriction from amniotic bands. In each case, the diagnosis was made retrospectively (1). Recognition of amniotic bands constricting the umbilical cord has been reported by Kanayama et al., who were able to document fetal compromise by reversal of diastolic flow in the umbilical artery by color Doppler (69). It is in cases like the one reported by Kanayama et al. that fetoscopic lysis of amniotic bands can be lifesaving.
The rationale for performing fetoscopic lysis of constricting extremity amniotic bands is based on the prenatal natural history that progressive compromise of fetal growth leads to amputation. However, this assumes that the procedure can be accomplished with no maternal morbidity and minimal fetal morbidity. This procedure is hard to justify in the face of a serious maternal complication or a fetal death due to severely premature delivery at 21 or 23 weeks of gestation, even in the face of certain fetal limb amputation.
There is no standard approach to fetoscopic lysis of amniotic bands and reports have ranged from single port to two port techniques using laser or endoshears to cut the band, respectively. These are extremely challenging fetoscopic cases as the amniotic fluid volume is normal or low and there is extensive disruption of the amnion with bands visible throughout, though not necessarily involving the fetus, but potentially obscuring visualization. All cases of ABS have disruption of the amnion and the fetoscope compounds this by adding puncture of the chorion to gain access to the baby. Involvement of an extremity can be difficult to treat unless the fetus is paralyzed with intramuscular injection of rocuronium as any touch of the involved limb will cause withdrawal of the limb.
Even in cases in which the fetus is paralyzed, the amniotic band has usually cut through at least the skin and subcutaneous tissues, if not muscle and tendon. In fact, ABS can result in fracture of the bones of the involved limb. The amniotic band is often deeply embedded in the depth of the wound caused by the constrictive band. Endoshears or a laser fiber can be used to cut the amniotic band which should then be removed circumferentially from the depth of the wound. Similarly, release of umbilical cord amniotic bands can be equally challenging as the bands tend to wear away Wharton’s jelly and the umbilical vessels are exposed deep to the amniotic band. In cuttting the amniotic band, either with endoshears or laser fiber, there is the risk of lacerating the underlying umbilcal vessels. In fetoscopic release of a symptomatic ABS, inspection of all fetal extremities and the entire length of the umbilical cord is indicated to exclude the presence of asymptomatic bands that are almost always found and should be released before they become severe enough to cause symptoms.
On the basis of their experience with fetoscopy for cord ligation in TRAP sequence and the experimental work by Crombleholme et al. demonstrating the potential for functional recovery of banded extremities once released, Quintero et al. performed the first fetoscopic lysis of amniotic bands in human fetuses (72,73). Their first case was a fetus at 21 weeks of gestation with bilateral cleft lip and bands attached to the face and left upper extremity with distal limb edema. In order to avert limb amputation, fetoscopic lysis of bands was attempted at 22 weeks of gestation using a two-port technique. However, because of bleeding encountered on insertion of the second operating port, it was removed and the lysis was performed under ultrasound guidance. There was resolution of the distal edema within 6 days of the procedure.
At 32 weeks, microphthalmia and anophthalmia of the right orbit were first noted at the site of the previously attached amniotic band. The infant was delivered at 39 weeks and was found to have a type IV Tessier craniofacial cleft and right microphthalmia. The extremity showed minimal residual scarring where the band had been attached and lysed. The infant’s hand had radial paresis and mild hypoplasia. The second case was a fetus at 23 weeks of gestation with a thick amniotic band constricting the left ankle of the fetus. There was marked edema distal to the band and minimal blood flow to the foot was observed by color and pulsed Doppler. Fetoscopy was attempted but bleeding was encountered on insertion of the operating port, necessitating its removal. Attempts at ultrasound-guided lysis using endoscissors were unsuccessful. A 2.4-mm 0-degree operating scope with a 400-μm contact YAG laser fiber was used to lyse approximately 85% of the band. The edema markedly improved, as did distal arterial blood flow, and there was return of flexion and extension on follow-up sonographic examination. The infant delivered at 34.5 weeks and underwent Z-plasties for residual effects of the amniotic band.
The experience reported by Keswani et al., similarly supports the use of fetoscopic release of amniotic bands for limb salvage (76). However, the sequelae of the ABS may not completely resolve or may result in secondary lymphedema.

Figure 6. Photograph of the hand of a baby with secondary lymphedema who underwent fetoscopic release of amniotic band at the wrist causing critical ischemia. The hand was saved but there was significant lymphedema as a consequence of the tourniquet effect of the amniotic band.
It is worth noting that the cases reported all had additional amniotic bands encircling limbs not appreciated by ultrasound examination that were also lysed. Snyder et al. reported their experience with expectant management vs. fetoscopic release of amniotic bands in 24 patients with 5 involving the umbilical cord (81). There were no differences in treated versus untreated ABS with regard to maternal age, parity, rate, diabetes, prenatally diagnosed abnormalities, distal deformity, lymphedema, and amputation. The severity of ABS appeared to be worse in the fetoscopically treated ABS, however, based on the higher rate of abnormal vascular flow (5/10 versus 1/13) and cord involvement (7/10 versus 1/13). The indications for fetoscopic treatment of ABS was the presence of lymphedema or abnormal extremity blood flow distal to the amniotic band, or the presence of cord entanglement.
Figure 7. Movie of fetoscopic release of amniotic band causing critical ischemia of the fetal left hand which was relased using Diode laser in contact mode.
The indications for treatment of additional unsuspected amniotic bands noted at the time of fetoscopy was the presence of the band encircling an extremity with or without distal findings and any involvement of the umbilical cord. Contraindications to fetoscopic release included the band not involving the cord or the fetus, causing severe encephalocele, or extremity amniotic bands in twins in which the procedure would put the uninvolved twin at risk. In contrast, umbilical cord ABS in a monochorionic twin would still be an indication in that the life and neurologic integrity of the uninvolved twin would be at risk in the event of the death of the baby with ABS involving the cord.
The median gestational age at delivery in the series reported by Snyder for the operative group was 29 weeks (range 25 to 34) vs 36 weeks (range 25-39) for those managed expectantly. The survival in the operative group overall was 80%, but 86% in the cases in which there was umbilical cord involvement. This is the largest single center experience with ABS treated by fetoscopic release and first successful treatment of umbilical cord ABS. There have been numerous individual case reports and one other small series of cases of ABS treated fetoscopically with similar findings (73-86). All cases of ABS are at risk for prematurity due to the disrupted amnion. However, the gestational age at delivery of ABS treated by fetoscopic release was significantly less than observation alone. Excellent survival in ABS involving the umbilical cord however, can only be achieved with fetoscopic release in which the natural history is usually associated with intrauterine fetal demise.
While extremity ABS may have devastating morphologic and functional effects on a limb, possibly resulting in amputation, it is not lethal. Extremity ABS is not an indication for fetoscopic surgery unless maternal risks and incidence of preterm labor are fully appreciated by the mother. However, there are forms of ABS that are lethal or have devastating neurologic sequelae that may justify the current risks of intervention. Torpin has reported 36 cases of constrictive amniotic bands of the umbilical cord, which were uniformly fatal (1). Although rarer than other forms of ABS, umbilical cord involvement, once diagnosed sonographically, is amenable to fetoscopic release to avert fetal death (69,81).
LBWC in the setting of monochorionic twins is also an indication for fetal intervention to protect the normal co-twin, due to the high rate of intrauterine fetal demise. LBWC complex is uniformly fatal but up to 50% will succumb to intrauterine demise as opposed to neonatal death. In monochorionic twins, LBWC in one twin puts the normal co-twin at risk for demise and severe neurologic injury in the event of intrauterine demise. The options for intervention in twins complicated by LBWC include selective fetoscopic laser photocoagulation of the communicating vessels on the chorionic plate to protect the co-twin or selective reduction by means of intra-fetal radiofrequency ablation of the cord of the fetus with LBWC. Which option is best may depend upon whether parents would be comfortable with selective reduction versus separation of the vasculature on the chorionic plate.
Postnatal Evaluation
A fetus known to have ABS should be delivered in a tertiary care center with Neonatologists, Pediatric Plastic and Reconstructive surgeons, and Pediatric Orthopedic surgeons available. Treatment depends on the nature of the ABS and the severity of the deformation. In cases of umbilical cord involvement, early or even emergency delivery may be indicated if there are signs of fetal compromise (69). After delivery, a careful physical examination should assess the severity of the ABS. Often there will be no evidence of the amniotic band at the time of delivery. In the case of extremity amniotic bands, treatment is dictated by the severity of the deformation. The severity of deformity can range from a mildly constrictive band, requiring release, to near amputation, requiring debridement. More often, there is a bandlike deformation that requires Z-plasties to surgically correct it (87-89).
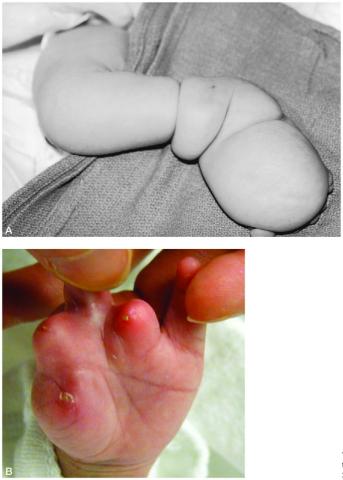
Figure 8. A. Postnatal appearance of the leg of a newborn with extremity amniotic band syndrome.
B. Postnatal appearance of the hand of a newborn with extremity amniotic band syndrome that resulted in digital amputation.
Postnatal Imaging
There is a limited role for postnatal imaging in ABS. However, in extremity ABS, plain radiographs should be obtained to rule out underlying boney fracture. If ABS results in encephalocele or facial clefts, ultrasound and MRI or CT scans should be obtained to assess impact of the bands on the central nervous system structures and craniofacial development with three dimensional reconstructions to assist in planning reconstructive procedures.
Medical Management
In cases of amniotic bands involving the face and head, there may be severe facial clefts, anophthalmia, and encephalocele. These deformities may require many extensive reconstructive procedures to achieve an acceptable cosmetic result. Cases of the LBWC form of ABS are always fatal, and no reconstructive procedures are indicated.
Outcomes
The outcome in ABS depends on the severity of the deformation. Cases of extremity ABS usually have an excellent long-term outcome. Even in cases of limb amputation, ambulation is possible with the aid of a prosthesis. The cosmetic results following extensive craniofacial reconstructive surgery are often acceptable, but the severity of these defects may leave these children permanently disfigured. ABS in which fetoscopic release was performed may show evidence of secondary lymphedema, which may require multiple surgical procedures to provide an acceptable functional result.