Congenital Epignathus
Congenital epignathus (from the Greek “epi” for “above” and “gnathos” for “jaw”) is an extremely rare form of teratoma (germ cell tumor) that arises from the oropharynx, the middle part of the throat, specifically from the hard palate. It is estimated that these tumors occur in approximately 1 in every 35,000 to 1 in every 200,000 livebirths (1). As a teratoma, all three primitive embryonal germ layers (endoderm, mesoderm and ectoderm) are present in these typically benign tumors that arise from Rathke’s pouch, which is an evagination or outpouching at the roof of the developing mouth in what will become the hard palate. Malignant or immature teratomas of the soft palate have also been reported and can include intracranial extension (2).
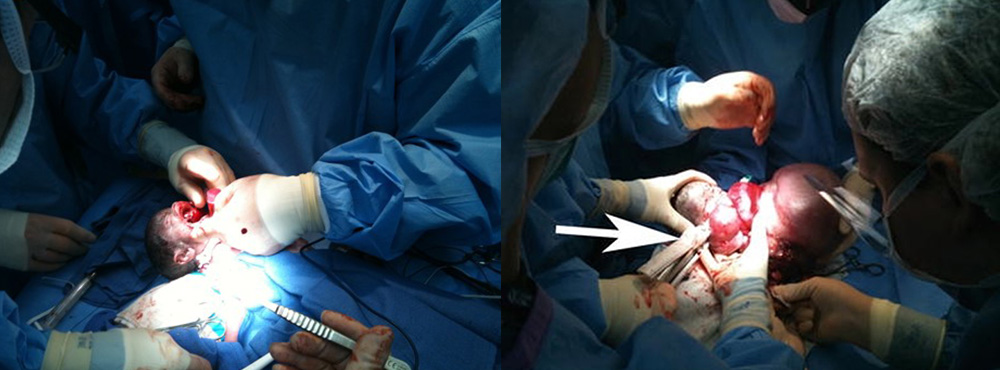
Congenital epignathus arise from the palate in the majority of cases and can be associated with cleft palate, tongue or nose anomalies (Figure 1) (3). Epignathus can grow to extremely large proportions but always has a narrow base arising from the palate with arterial blood supply solely from one or both palatine arteries. The mass may grow at such a fast rate that it can distend the mouth, causing mandibular dislocation of the temporomandibular joints bilaterally. The blood flow in these large epignathi may be sufficiently large to cause high output cardiac failure. Tumors sufficiently large to cause this volume of blood flow can literally “steal” from the baby causing growth arrest.
Epignathus tumors may be relatively easy to diagnose at birth but tumors have been diagnosed prenatally using real-time ultrasound for decades (4). Prenatal diagnosis can be critical as large epignathus can lead to airway obstruction and high mortality rates (5, 6).
In a review by Clement of cases reported in the literature between 1989 and 1999, 15 cases of epignathi were summarized (7). All but three were prenatally diagnosed and ranged in size from 2 to 17 cm. Cases were diagnosed in all trimesters but the majority were the third trimester. Of the cases that reported outcomes, 5 resulted in a perinatal death and 3 were elective terminations.
Prenatal detection of oropharyngeal tumors is primarily by ultrasound. Detection of epignathus may be aided by development of polyhydramnios, due to obstruction of swallowing prompting referral for ultrasound. In some cases, the epignathus may be functional secreting the tumor marker alpha-fetoprotein which may prompt referral for ultrasound. A case of congenital epignathus associated with a maternal serum alpha-fetoprotein (MSAFP) of 7.7 MoM at 15 weeks was reported leading to prenatal diagnosis by ultrasound at 17 weeks (7). In another case of elevated MSAFP of 5.1 MoM at 19 weeks ultrasound revealed an epignathus teratoma was also reported (8).
Congenital Epulis
Congenital epulis (from the Greek “epi” for “above” and “oulon” for “gum”) is a rare oral tumor arising from the alveolar ridge of the maxilla or mandible. These tumors, first reported in 1871 by Neumann, are granular cell tumors (9). The differential diagnosis includes hemangioma, fibroma, teratoma and granuloma. In an extensive review of the literature, Zuker reported on 195 lesions diagnosed starting from 1871 (9). The majority of cases were in females (10 to 1) and the tumors were twice as likely to be maxillary in origin, usually in the incisor or canine region. These lesions are typically solitary but can be multiple, smooth pedunculated tumors that range from several millimeters to many centimeters in size. Histogenesis of the tumors is uncertain but the predilection for females suggests a hormone sensitive tissue of the origin. Postnatal observation of epulis tumors often show progressive involution (shrinkage) consistent with hormonal influence with withdrawal of pregnancy related hormonal milieu. The histology of epulis is similar to other granular cell tumors (10).
Ultrasound is the primary mode of detection of congenital oropharyngeal tumors such as epignathus and epulis. Epignathus can have a varied presentation by ultrasound. The tumors tend to be complex with cystic and solid components and color-flow Doppler can demonstrate blood supply from the palatine arteries (Figure 3.). Epignathus, being a teratoma, has a greater propensity to grow to significant dimensions. Due to their origin in the hard palate when they enlarge, they obstruct the fetal airway and may distend the mouth to the extent that the temporomandibular joints become dislocated. Both 2-D and 3-D ultrasound have been used to diagnose and characterize congenital epignathus (14, 15, 16). Shih reported using 3-D ultrasound reconstruction of the upper airway to virtually determine if intubation could be possible in a case of epignathus. In this case, MRI confirmed the diagnosis and probable airway compromise, and an EXIT procedure was planned due to the extent of the tumor.
Figure 1
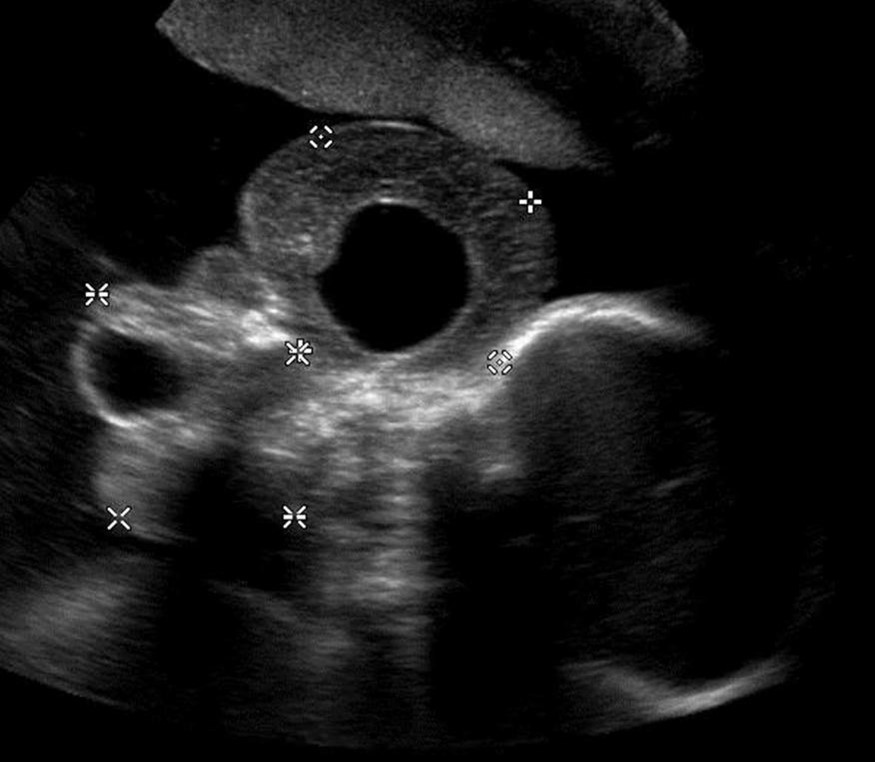
Congenital epulis typically arise in the second or third trimester. They appear as well-defined round masses near the naso-labial junction arising from the alveolar ridge of the mandible or maxilla but commonly from the maxilla (11, 12). The vast majority of congenital epulis are solitary although numerous cases of multiple lesions have been reported (Figure 2) (13). Unlike epignathus, epulis tends to be smaller, may be multiple and compromise of the airway is less common. Increased blood supply through a vascular pedicle is typical. No other fetal anomalies have been reported to be associated with congenital epulis but the differential diagnoses when prenatally detected includes other oral-facial masses such as hemangioma, sarcoma, and granular cell myoblastoma.
Figure 2
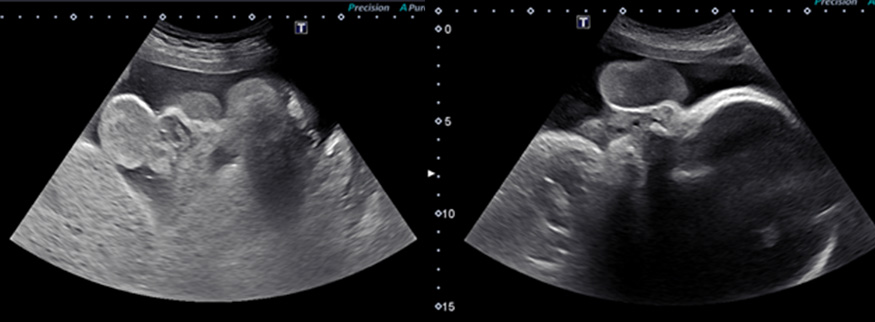
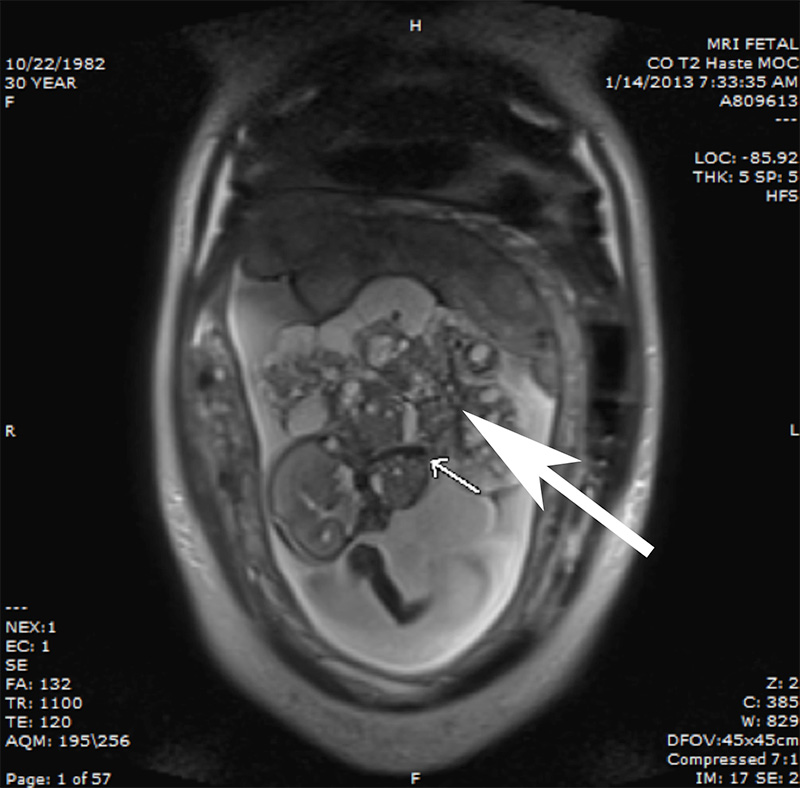
Accurate prenatal diagnosis and establishment of the extent of a congenital epignathus or epulis is important to plan for delivery room management. The use of 3-D ultrasound has been described in the evaluation of facial masses, but MRI may be more helpful in elucidating the origin of facial tumor (15). Due to the larger field of view with fetal MRI, a better appreciation of the dimensions of the epignathus and the narrow base on the hard palate can be obtained (Figure 3). If blood flow to the epignathus is sufficiently large, the flow voids caused by the palatine arteries can be visualized (Figure 3).
Figure 3
MRI has also aided in the diagnosis of congenital epulis (15). On MRI, epulis tends to be a discrete mass with smooth borders arsing from the ginginva (17). Roy and colleagues reported a case of congenital epulis that was diagnosed at 38 week’s gestation by prenatal ultrasound (18). Two small lesions were noted to be protruding from the fetal mouth. Fetal MRI using a HASTE sequence confirmed the diagnosis of epulis showing homogeneous tumors of low signal intensity on T1-weighted images arising from the mandible and maxilla. Congenital epulis tends to have isointensity with muscle on T1-weighted imaging and isogeneous to heterogeneous signal intensity on T2-weighted imaging (19). Additional reports indicate congenital epulis can display a similar signal to muscle on T1-weighted imaging or iso- to heterogeneous signal intensity on T2-weighted imaging.
A possible limitation of MRI is that it cannot provide functional information on possible airway obstruction after birth. In the absence of polyhydramnios, preservation of fluid in the oropharynx has been used on MRI to suggest that the airway has not been compromised (16). Bornstein and colleagues described sonographic functional assessment of congenital epulis including fetal breathing and swallowing, presence and severity of polyhydramnios or an absence of a stomach bubble, and bidirectional flow of fluid from the nares to assist in deciding airway compromise and delivery room management with the need for a possible EXIT procedure (19). We view ultrasound and fetal MRI as complimentary imaging modalities essential in determining the appropriate delivery management of epignathus and epulis.
There are several options for fetal intervention in epignathus and epulis. Epulis rarely becomes so large as to cause polyhydramnios or high output failure during mid-gestation. More often, in epulis, the mass is modest in size and does not compromise the fetal airway. Epignathus, in contrast, can grow to enormous proportions sometimes the size of the entire fetus. Decision-making in the management of epignathus will depend on gestational age, presence or absence of polyhydramnios, high output state, signs of hydrops, growth restriction and evidence of fetal airway compromise. Patients less than 30 weeks’ gestation with these complications are at risk for intrauterine fetal demise, preterm premature rupture of membranes, preterm labor and delivery with attendant risks of prematurity.
Fetal surgery has been reported for epignathus. Kontopoulos reported a case of isolated epignathus with no evidence of spread (25). A feeding artery was identified by Doppler ultrasound and tumor resection was accomplished by fetoscopic transection of the stalk. Caution is advised for fetal treatment as there can be associated clefts and extension of the tumor not appreciated by fetal imaging. Especially when epignathus presents in association with cleft palate, one should consider the impact of treatment on the palatal blood supply upon which the palatal flap for cleft palate repair will depend. Other pregnancy management may include therapeutic amniocentesis for cases of severe polyhydramnios or premature delivery for cases of hydrops (21).
Ultrasound guided intravascular coagulation is a less invasive approach to treating giant epignathus complicated by hydrops, high output failure, or growth restriction from vascular steal. This approach has been used successfully in the management of bronchopulmonary sequestration and sacrococcygeal teratoma in selectively devascularizing the tumor (26). Epignathus is uniquely suited to this form of intervention as the mass derives its entire blood supply from the palatine arteries. These feeding vessels can be demonstrated within the mass by color Doppler in cases manifesting complications related to large volume of blood flow. An 18-gauge needle can be ultrasound guided to the palatine artery at the base of the tumor and a 600-micron Endostat advanced into the vessel and photocoagulated. The palatine arteries should be treated within the exophytic mass of the epignathus to avoid vessel rupture and hemorrhage as well as compromise of the blood supply of the palate. This can be repeated within the tumor to treat branches of the left and right palatine arteries until the exophytic portion of the epignathus is completely devascularized. The interruption of blood flow to the tumor will normalize the combined ventricular output and eliminate vascular steal. Necrosis of the mass will result in progressive reduction in the size of the mass and improvement in polyhydramnios. As the gestation progresses, ongoing assessment for the need for EXIT strategy for delivery is important as the size of the residual mass may still compromise the airway.
After 30 weeks’ gestation, if hydrops, severe polyhydramnios, vascular steal, or high output state with combined ventricular output greater than 600 ml/kg/min develops, serious consideration should be given to EXIT-to-Resection. The narrow base of origin on the hard palate in epignathus makes even a very large exophytic tumor relatively easy to deal with by stapling across the base of the tumor with a thick tissue GIA stapler (Figure 4). Depending upon the maternal-fetal stability, a complete resection of the residual tumor from the palate can be performed during the EXIT procedure or can be deferred until after the baby is stabilized following delivery.
Figure 4