Fetal alloimmunization, previously referred to as isoimmunization, occurs when a pregnant person’s immune system produces antibodies against fetal red blood cell antigens which can attack and destroy the fetal red blood cells (hemolytic anemia).
Background
Every individual has red blood cells that are responsible for transporting oxygen from the lungs to the tissues of the body. Red blood cells have multiple different types of inherited antigens, which are proteins or carbohydrates present on the red blood cell surface. These antigens define our blood type and immune response. Most commonly we understand these as ABO antigens. For example, people with type A blood have A antigens, type B have B antigens, Type O blood has neither, and AB has both. Some red blood cell antigens are well known (for example Rhesus antigens which can lead to Rh disease due to the presence of Rh D antigen), and other lesser known but clinically important antigens (Kell, Kidd, and Duffy). There are over 300 known red blood cell antigens.
Pregnant patients can become sensitized to foreign antigens through exposure to blood transfusions, pregnancy and childbirth, and any other form of foreign blood component contamination.
Identification of a maternal antibody response to fetal red cell antigens and follow-up screening allows for treatment, and sometimes even prevention, of fetal alloimmunization in pregnancy. Depending on the antigen type, antibody formation and transplacental passage, there can be significant risks to the fetus leading to hemolytic anemia (when the attacking immune system causes the breakdown of fetal red blood cells), heart failure and stillbirth. Most commonly this is seen in Rh Disease, which can cause devastating anemia in the fetus. The introduction of Rhogam in the late 1960s has dramatically reduced the incidence of fetal death among patients with Rh Disease to 1-2%.
At the Fetal Care Center at Connecticut Children’s, we screen for and manage cases of alloimmunization in order to preserve the life of the affected fetus. Below are some common questions patients may have as they navigate a pregnancy complicated by alloimmunization.
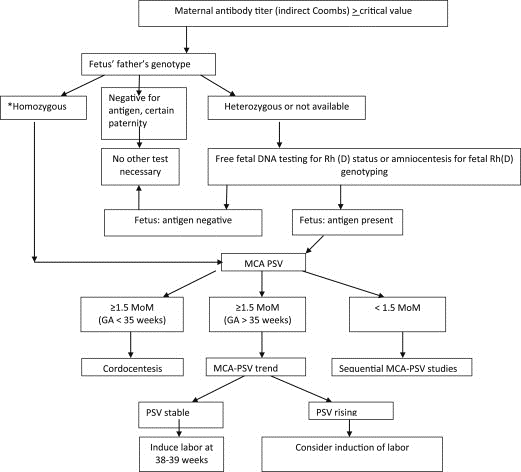
In the majority of cases where there is a known maternal antibody and a concern for discordant paternal antigen, titers can be followed. This is usually performed monthly in early pregnancy with the interval shortened in the case of changes or concerns. Antibody titers measure the concentration of an antibody in the maternal serum—it is done with serial dilutions of 1:2 until no further antibody can be detected. For instance, at a titer of 1:8, antibody was still detected after dilution of 1 part serum to 8 parts of a solution. Higher antibody titers correlate to a stronger antibody response with more antibodies present (this in turn increases the likelihood of transplacental passage and resultant hemolysis and fetal anemia). A critical titer in most institutions and for most antibodies is usually between 1:16 to 1:32. When this critical titer is reached, middle cerebral artery (MCA) Doppler assessment is initiated. (This is generally not initiated until after 16 weeks of gestation).
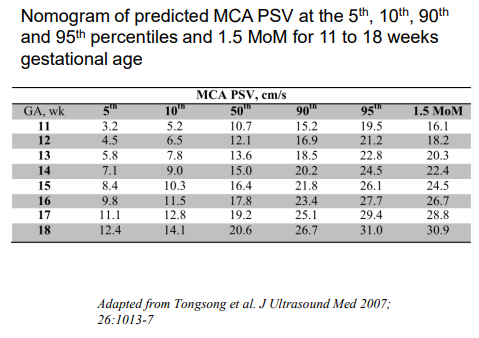
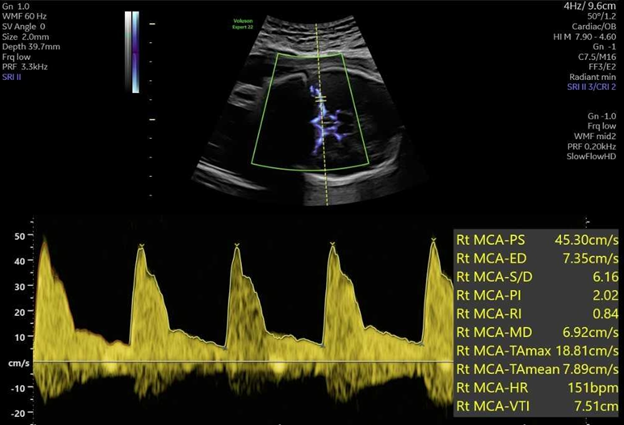
MCA Dopplers rely on measurement of the peak systolic velocity (MCA-PSV), or speed the blood travels through a vessel in the brain, to detect fetal anemia. Velocities are gestational-age dependent and a value greater than 1.5 MoM or multiples of the median correlates to increased risk for fetal anemia. It is important to have MCA-PSV completed in a center well trained in obtaining these measurements, such as with the Fetal Care Center at Connecticut Children’s, because they are highly dependent on the ultrasound angle of insonation, and can be affected by fetal movement and heart rate accelerations (Crombleholme). They can also be affected by later gestational ages, and earlier gestational ages require specific algorithms (See Figure 1).
Figure 1
Overall, there is a 12% false positive rate, which is more frequent after former fetal transfusions. Some more recent studies have also looked at cardiac function assessment with 73% of providers in the international expert Delphi consensus on monitoring and management of hemolytic disease reporting utilization of cardiac size and valvular regurgitation as parameters to assess fetal anemia, though not to guide management such as with intrauterine transfusion. In red cell isoimmunized pregnancies, the left and right cardiac output is increased in proportion to the degree of fetal anemia.
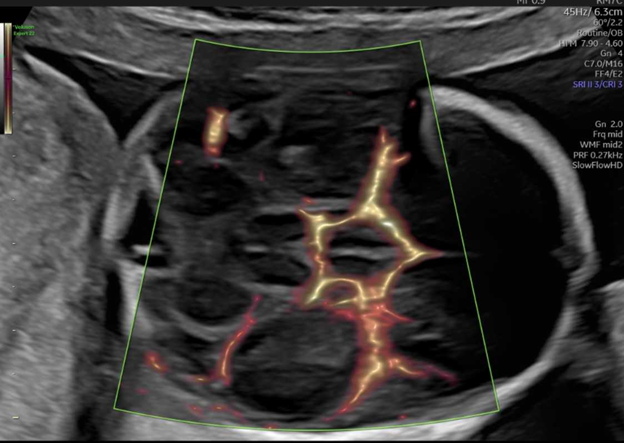
MCA Dopplers (see Figure 2) are usually initiated at 16 weeks of gestation (though in some cases may be performed as early as 15 weeks). If there is a true fetal anemia suspected after MCA Doppler surveillance, the next step is to proceed with percutaneous umbilical vein sampling (PUBS) and intrauterine transfusion (IUT). During this procedure, fetal blood is sampled through the umbilical vein and hemoconcentrated, leukoreduced, irradiated CMV negative blood is transfused into the fetus to bring the hematocrit (HCT) to at least 45 (40-50 g/dL). Generally, a goal hematocrit of 75-80% should be achieved in the blood sample for transfusion in order to reduce the volume of blood needed to infuse into the fetus, and decrease risk of fetal compromise from volume overload and increased strain on the fetal heart.
Figure 2
Umbilical vein access is best obtained at the placental cord insertion, followed by a free floating loop of cord or the intrahepatic vein alternatively. Umbilical vein insertion into the abdominal wall is generally avoided due to concern for possible fetal bradycardia. Generally PUBS is reserved until after 20-22 weeks gestation due to higher risk of fetal complications at earlier gestations, however, intrahepatic and intraperitoneal transfusions can be performed even as early as 17 - 18 weeks in special cases.
Some centers may follow MCA-PSV after the first one or two transfusions to guide subsequent transfusion timing, though MCA Dopplers may be less reliable after multiple transfusions of adult red blood cells. They may also be less reliable later in the third trimester. More commonly, there is a recommended interval by which further transfusions can be guided based on anticipated decline in fetal hemoglobin over time (generally thought to be about 1g/dL every three days). Some centers will use empiric intervals to time transfusions.